My new neighbor and friend, Suzanne Edwards, who arrived from England only two weeks ago, just underwent a successful spinal cord surgery to remove a large arachnoid cyst that was pressing on her spinal cord. She’s been a great patient and is recovering quickly.
During Suzanne’s surgery, chief neurosurgeon Dr. Liu also discovered multiple bone fragments left alongside spinal cord by her original surgical team in England. So this surgery turned out to be more important for Suzanne than she may have imagined. Indeed, Dr. Zhu reported that the pressure inside Suzanne’s cyst was even greater than my own very high pressure in May.
It is unfortunate that in the United States and many other countries so many neurosurgeons are reluctant to operate inside a spinal cord, perhaps due to lack of experience with this admittedly tricky procedure. The problem with cysts in or near the spinal cord is that often they continue to grow by filling up with fluid and building up pressure that results in reducing a person’s functionality as well as causing severe pain. In my case, for example, an ascending cyst in my cervical spinal cord had already started to affect my breathing, not to mention causing intractable neuropathic pain.
In much of the developed world, neurosurgeons pretty much despair of helping spinal cord injury patients, especially those that are labeled “complete” injuries. These surgeons seem to conclude up front that most SCI patients will not regain motor function after surgery, and, therefore, the so-called standard-of-care is only to secure the broken vertebrae in what is known as a “spinal fusion” — which is essentially an orthopedic procedure that mechanically reinforces the spinal column.
In contrast, experienced Chinese neurosurgeons not only deal with mechanical stabilization but also open the spinal cord in newly injured patients to reduce as soon as possible the build-up of inflammatory pressure from the injury. This strategy results in much less secondary injury and consequent sparing of axons that would otherwise die off. And this decompression strategy apparently explains why many Chinese SCI patients are able to benefit so much from rigorous rehabilitation, as I have repeatedly witnessed here in Kunming.
Unfortunately, in Miami I did not have the benefit of such progressive surgery, and thus I suffered typical secondary injury that killed off axons that might otherwise have lived. Consequently, I have not so far benefitted from the Kunming “walking” rehab program.
Thus my primary goal now is to somehow reduce my persistent, severe pain levels.
A few days ago I was speaking by telephone with my Dad, who was in the Netherlands attending an international pain research conference spnsored by the IASP.
http://www.iasp-pain.org/am/template.cfm?Section=Home
Dad is presently on his second round-the-world “pain tour” as dealing with my incapacitating pain, and no longer physical rehabilitation, has become our top priority.
I mentioned to Dad that even if I regain no motor function during my time in China, as seems probable at this point, it will still have been worth coming over here, because my surgery was pretty much a life or death situation. Before surgery the cyst had grown 30% in the prior 18 weeks and had started to impair my breathing. So, a few months more and who knows what would have happened.
When you live with a major spinal cord injury and suffer every single day from a combination of severe neuropathic pain + allodynia … well, as I’m sure many of my readers can relate, walking no longer seems as important anymore as reducing systemic pain to a level where you could visualise having a meaningful life.
Maybe the best way to explain how long-term pain affects your brain is to consider having insomnia for a long period of time, say getting by on just 2 to 3 hours of sleep a night. After a while, you start to hallucinate, can barely form sentences and feel like you’re going crazy. Long-term neuropathic pain kind of works the same way. It deprives you of sleep and over time just wears you down to the point where you can barely function.
With respect to the neuropathic pain, we are getting that much closer to finding a solution to importing the reagents needed to test lithium blood serum levels. The challenge is that the lithium reagents need to be refrigerated, and we do not want them to get stuck in customs. It has been a longer process than we anticipated, but are hopeful we can start in the next month or so.
As an alternative to drugs, I will be spending the next six weeks attempting to remap my brain so that my brain interprets pain signals in a less hostile and debilitating way. In the next week or so, I will dedicate an entire blog to how I’m going about remapping my brain to down-regulate its perception of pain.
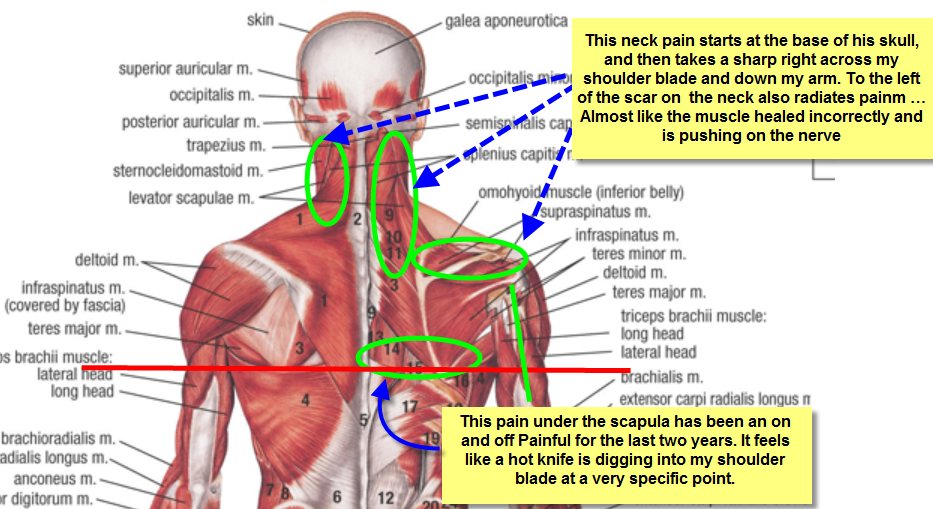
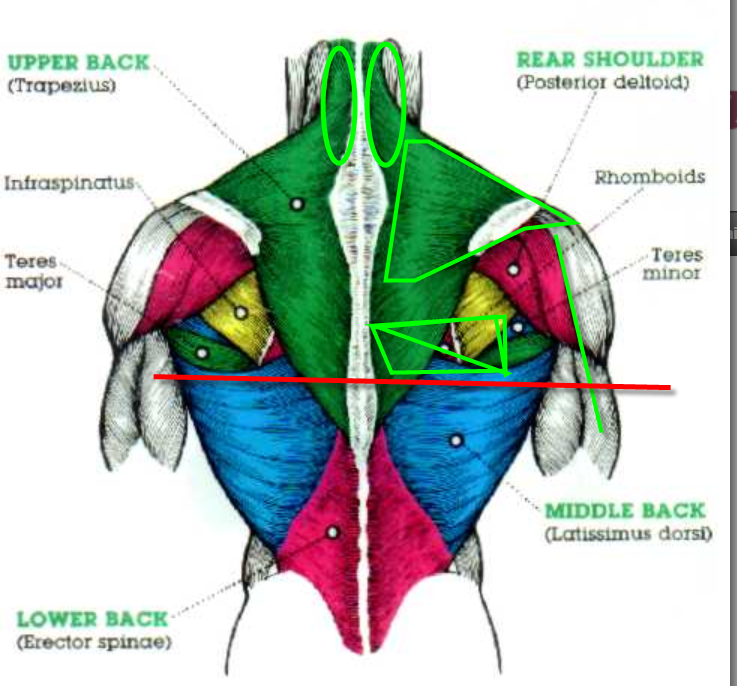
Otherwise, I believe we have narrowed down the issues I’m having with intense shoulder and neck pain radiating pain down my right arm. It looks like I may have several pinched nerves in the C5-C7 area where I had my surgery this past May.
What I am experiencing feels like a radiating hot pain from my neck down to my shoulder blade and then over to my right shoulder and down my right arm. Throughout that area, it feels like somebody’s taking a knife and cutting open my muscles.
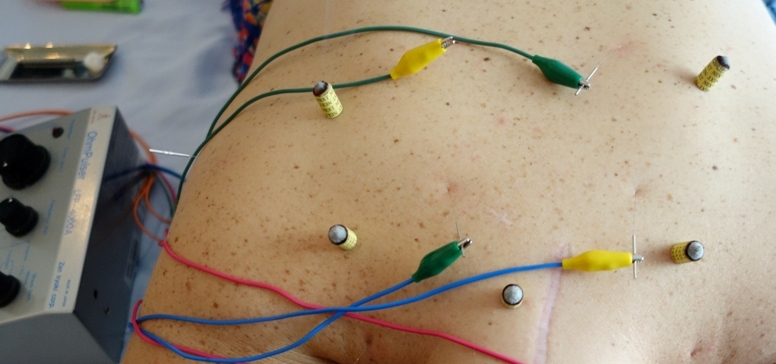
When there are pinched nerves involved, these damaged nerves can actually alos weaken the muscles they control, and it feels like multiple pulled muscles at the gym. I’m working with several doctors in the United States to get to the bottom of this post-surgical injury, and if we find a solution I will follow up with e fuller account. In the meantime, I’m still working with Ericko here in Kunming on electro-acupuncture and massage to ease the shoulder injury.

I will post the Part II blog in the next few days and get into a little bit more detail about how I’m planning to shift my life focus in the months just ahead.