Cervical Vertebrae
I’ll do my best to describe my upcoming surgery — finally now scheduled for May 14th. I hope the illustration here helps a little, as this is pretty complicated to describe without a visual. In fact, in my Dad’s meeting with our Kunming neurosurgical team and core advisers last week, he had the benefit an actual skeleton that enables a 3-D understanding of the surgical procedure.
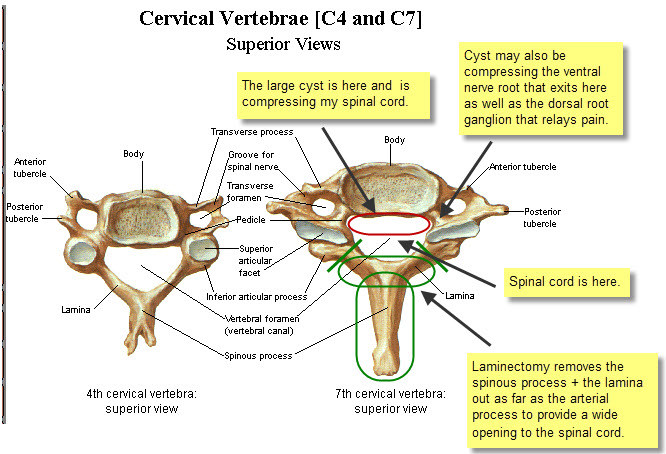
Anyway, the objective here is to reach the fluid-filled cyst on the anterior (front) side of my spinal cord in order to cut it open and drain the fluid, thereby decompressing my spinal cord.
My 2010 spinal fusion involved screwing a metal plate between the C-5 vertebra and C-7 vertebra, because my C-6 vertebra burst in the diving accident. Therefore, access to my anterior cyst is blocked on the ventral (front) side of my spinal column due to the metal plate being in the way. So Dr. Liu will have to access the cyst from the back side – “dorsal entry.”
To gain access to my spinal cord, the surgeon needs to create as wide an opening as possible. This surgical procedure is referred to as a “laminectomy” because it involves removal of as much as possible of the lamina (bone) on both sides. However, because a major artery passes through the articular process on either side of the lamina, there’s a limit to how far the surgeon can go – roughly indicated by the angled green lines shown above.
And executing this triple laminectomy is just the “easy part” … 🙂
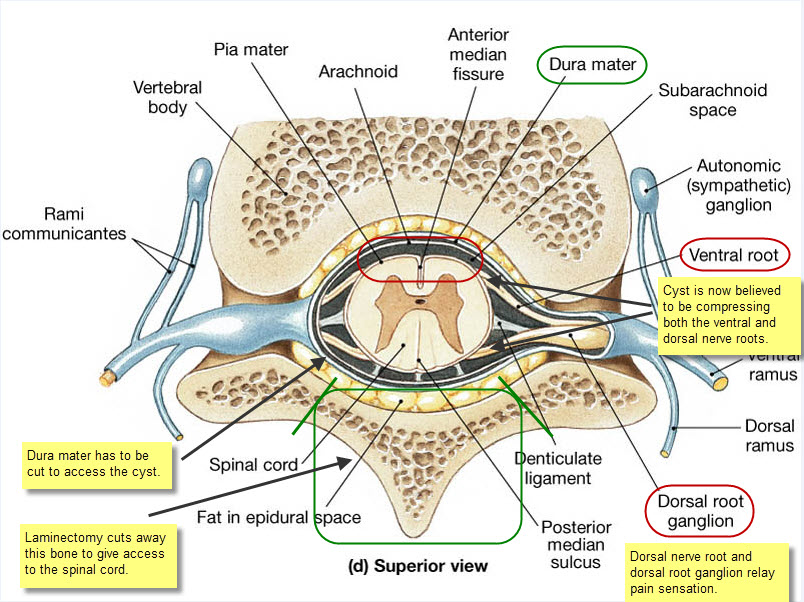
Next, the chief neurosurgeon, Dr. Liu Yansheng, will have to decide whether to approach the cyst by making his way to the left or right around my spinal cord. Once a path has been decided, he will have to cut open the Dura mater and then cut ligaments that hold the spinal cord centered, pushing aside my spinal cord very, very gently as he goes. I hope the following illustration gives you some idea of what’s involved here.
Vertebra Cross Section
Now comes the super tricky bit … absolutely no room for error or I’m toast.
Once Dr. Liu has worked his way round to the cyst, which is now relatively much larger than illustrated here, occupying about half my spinal canal, he cannot simply remove it because of the risk of tearing the Pia mater that encloses what remains of my spinal cord. So he’ll have to cut the cyst longitudinally, sort of like slitting a balloon so it can never again hold water.
Along the way, Dr. Liu will also scrape away and remove scar tissue from my original injury, thereby “untethering” my spinal cord and restoring CSF (“Cerebral Spinal Fluid”) circulation.
Dr. Xu Xiao-Ming, Professor of Neurological Surgery at Indiana University, expresses the strategic surgical concept as follows: “The key goal here is restoration of spinal morphology.”
Put another way, the goal is to restore my spinal cord as close as possible to its original design and orientation within the spinal canal. That means my spinal cord will no longer be compressed by the large cyst nor will it be tethered by strands of scar tissue left behind from my original spinal fusion surgery. Instead, my spinal cord will be floating free again with full CSF circulation — free once again, as Dr. Zhu Hui expresses it more poetically, to “dance” with the rhythms of my heartbeat and breathing. 🙂
Restoration of free CSF circulation, being no longer impeded by either scar tissue tethering or cyst, together with spinal cord de-compression by draining of the large cyst … these advances are both believed to be critical to achieving the optimal results from the Kunming Walking Programme. But at this point, frankly, I’d settle simply for cessation of the persistent severe neuropathic pain that makes it pretty much impossible for me to focus on anything else.
Now, of course, cutting away so much bone critically weakens the spine, and in my case the surgeon will have cut away altogether significant parts of three vertebrae … C-5 through C-7.
So once this access “door” has been cut open, there’s an obvious need to build a frame around the opening to reinforce the spine. This requires the installation of titanium rods and screws – two vertical rods and one horizontal rod to provide lateral rigidity, held in place by six screws.
After the cyst has been cut and tethering scar tissue removed, the Dura mater is sutured back together, and then the titanium rods and screws are installed. Then my neck muscles will be pulled back over the titanium framework, and finally they’ll suture my skin back in place.
Two or perhaps three days in intensive care are followed by two weeks of bed rest. After about 15 days, I will be expected to rejoin the Kunming Walking Programme!
My great new friend, Nu Jia, from Guangzhou, underwent pretty much identical surgery with Dr. Liu on February 18, 2012, and she was actively enrolled in Dr. Zhu Hui’s rehabilitation programme by March 8th. The idea here is that robust rehabilitation is key to rapid recovery and eventual restoration of useful motor function.
The great team of advisers who have helped me make the decision to go ahead with all this include my tireless Dad + Dr. Liu Yansheng (Kunming Tongren Hospital chief neurosurgeon ) + Dr. Zhu Hui (Kunming Walking Programme founder) + Dr. Wu Wutian, M.D., Ph.D. (Hong Kong University Professor of Neuroscience) + Dr. Xu Xiao-Ming, M.D., Ph.D. (Indiana University Professor of Neurological Surgery).
Frankly, I’m at a loss how to express my gratitude to Dr. Zhu Hui and to these busy men for the work and time they’ve contributed to spell out for me the complexity and risks of this undertaking. That said, I’m also deeply appreciative of how relaxed Dr. Liu appears to be about a procedure he has performed successfully many hundreds of times! 🙂
On a final note, I would not have been able to write this blog entry without my Dad. Well, let’s be frank, I would not be in Kunming if it were not for my Dad. My Dad’s energy is far greater than any young person I’ve ever met and he is simply my hero!

Working Group

“Hominid Wu” 🙂

Lighter side of Dr. Wu

Dr. Liu & Dad

Surgery Dialogue

This is such exciting news Ali! You are getting close! Miss you. X
I will be praying for you on May 14, 2013 for a successful operation. My husband wasn’t as fortunate. The key is to destroy as little as possible the nerve ending conductors. That is where his problem lies. The nerve endings that were damaged from his fall and his neck decompression operation never had a chance to regrow. God be with you and your surgeons.
you my friend are a global trailblazer. Will only be thinking and visualizing positive outcomes, a smooth operation, following by you standing strong and tall and walking. Let’s all keep the picture ! It’s happening baby, your just going through the STEPS now
Love Hominid Wu! And three cheers for your dad, he is amazing! Pretty soon your spinal cord will be dancing with your heartbeat for the first time in 3 years!!!