I apologize that it has taken me two weeks to post the third installment of my anniversary analysis of my experience here in Kunming, China.
Unfortunately, I developed another pressure sore, so I was stuck in bed for a week flipping back and forth. To add insult to injury, one of my porcelain tooth inlays fell out. Believe-it-or-not, my amazing friend Jenny managed to arrange for a city-center dentist to come all the way down to my apartment to glue the tooth back together!
As you can see from the picture it was a comedic/terrifying event, albeit the tooth has been reset quite unevenly and will have to be rebuilt with a crown. But how extraordinary that a busy dentist here in China could be persuaded to make a house call …
🙂

At-Home Dental Office!
Today I’ll focus on spinal cord surgery at Tongren Hospital and on the personal experience I had here a year ago in May 2013.
In fact, I’ve decided to break my report on surgery into three sequential blog entries, otherwise you might be reading for a couple hours today:
- Spinal surgery
- Immediate post-operative care
- Long-term post-surgical complications
It is quite common for spinal cord injury patients to develop over time one or more internal spinal cord cysts. Some SCI patients go their entire lives without realizing they have cysts, but they are lucky that these fluid-filled cysts do not affect their daily lives. Unfortunately, I was not so lucky.
About six months before I moved to Kunming, an MRI revealed that I had at least one large “arachnoid cyst” wedged between the Dura mater and my spinal cord. We sent my MRI to several neurosurgeons, who expressed different views on whether my cyst was affecting motor function, breathing and whether or not my spinal cord was actually tethered, which is quite common for many SCI patients. Several neurosurgeons claim not to have observed anything, and one even said the cyst was growing inside my spinal cord!
In much of the world, neurosurgeons decline to operate inside the Dura mater, especially for those patients judged to have “complete” injuries. These surgeons seem to feel that most SCI patients will not regain motor function after surgery, and, therefore, the so-called Standard-of-Care is only to secure the broken vertebrae in what is known as a “spinal fusion” – which is essentially an orthopedic procedure that mechanically reinforces the spinal column but does not involve dealing with the internal spinal cord inflammation, which is actually the main reason so many neurons die off during the days immediately after injury.
My Dad, ever the detective and usually unimpressed by much of what passes for conventional wisdom in the medical world, flew over to Kunming multiple times to meet Chinese neurosurgeons, first at the Peoples Liberation Army hospital and later at the private Tongren Hospital to discuss my case.
In particular, he focused on two doctors who have decades of experience with thousands of spinal surgeries and have removed all sorts of cysts within the spinal cord as well as performing un-tethering surgeries for patients. They have both recently retired from military service and taken up appointments at the private Tongren hospital.
By the time I finally arrived in Kunming in March 2013, the largest of my spinal cysts was growing rapidly and ascending into the C4 area … and was beginning to choke off my breathing!
So I definitely needed spinal surgery, and it appeared to us that this Chinese team had the most experience with my particular problem, which had become life-threatening.
My Kunming medical team leadership (Drs. Liu Yansheng and Zhu Hui) concluded that the combination of my “tethered” spinal cord + a 3.5 cm fluid-filled cyst growing on the anterior (front) side of my spinal cord (running from C-4 down to my C-7 vertebra) needed to be dealt with urgently, alone for me to regain control of my breathing. Further, there was MRI evidence that the rising internal pressure was also causing further degeneration of surviving tissue inside my spinal cord.
The surgery proposed turned out to be seriously tricky because the cyst was on the anterior (front) side of my spinal cord, whereas surgical access is only possible from the back side … known as dorsal entry.
This means that between the point of surgical entry and access to the cyst no less than three intact vertebrae had to be cut away, but also the actual spinal cord itself was in the way. Some obstacle course!
We have learned that few neurosurgeons anywhere in the world have working experience with a procedure this complex — some would say even “daring” – and even fewer apparently would be willing to attempt it, especially in the United States with lawyers and insurance companies complicating doctors’ work.
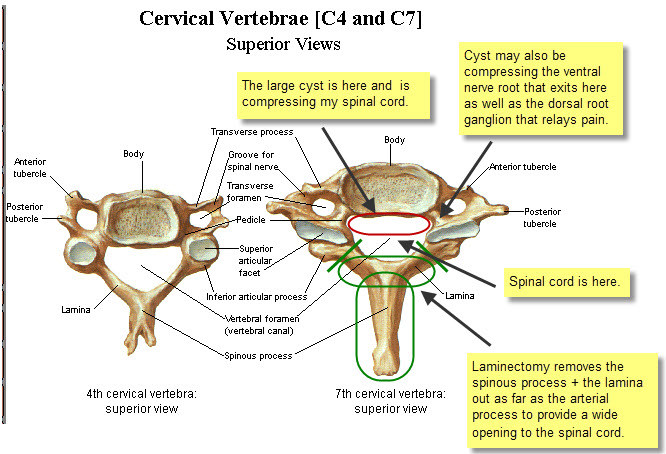
Cervical Vertebrae
Anyway, the objective was to reach the fluid-filled cyst on the anterior (front) side of my spinal cord in order to cut it open and drain the fluid, thereby decompressing my spinal cord.
My 2010 spinal fusion in Miami had involved screwing a metal plate between the C-5 vertebra and C-7 vertebra, because my C-6 vertebra burst in the diving accident. Therefore, access to my anterior cyst was blocked on the ventral (front) side of my spinal column due to the metal plate being in the way. So Dr. Liu had to access the cyst from the back side – “dorsal entry.”
To gain access to my spinal cord, the surgeon needed to create as wide an opening as possible. This surgical procedure is known as a “laminectomy” because it involves removal of as much as possible of the lamina (bone) on both sides. However, because a major artery passes through the articular process on either side of the lamina, there’s a limit to how far the surgeon can go – roughly indicated by the angled green lines shown above.
And successfully executing this triple laminectomy was just the “easy part” … 🙂
Next, lead neurosurgeon (of the four altogether who worked on me) Dr. Liu Yansheng had to decide whether, after opening the Dura mater, to approach the cyst by making his way to the left or right around my spinal cord. He decided to go right, then cutting through ligaments that hold the spinal cord centered, pushing aside my spinal cord very, very gently as he went along. I hope the following illustration gives you some idea of what’s involved here.
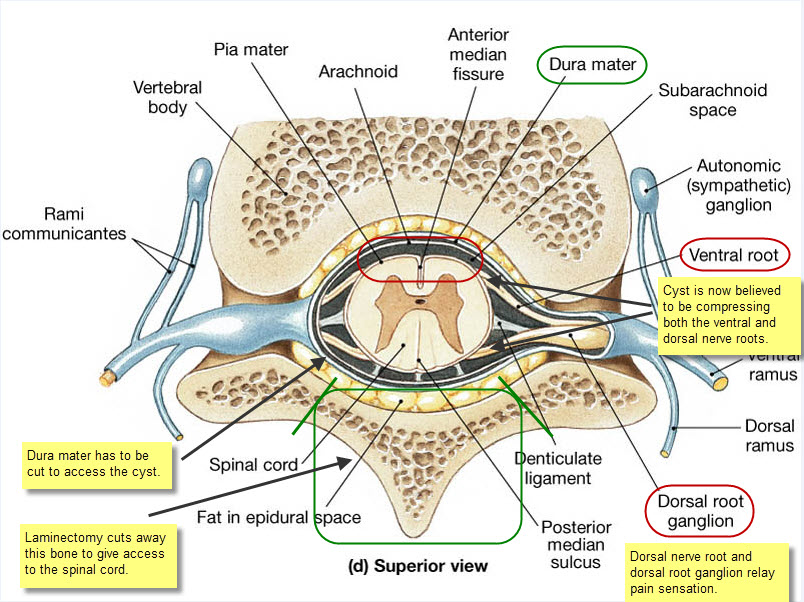
Vertebra Cross Section
Vertebra Cross Section
Now came the super tricky bit … absolutely no room for error here or I would have been toast.
🙂
Once Dr. Liu worked his way round to the cyst, which turned out to be relatively much larger than illustrated here, occupying half my spinal canal, he could not simply remove it because of the risk of tearing the Pia mater that encloses what remains of my spinal cord.
So he had to cut the cyst longitudinally, sort of like slitting a balloon so it can never again hold water. Once he was inside the Dura mater, he also discovered a couple more small cysts (a type called a syrinx) that had grown just inside the surface of the Pia mater, which had not been revealed in the MRI. Dr. Liu had to delicately lance this cyst, taking extreme care not to further damage my spinal cord, of which he estimated about 30% remains healthy.
Along the way, Dr. Liu also scraped away and removed scar tissue from my original injury, thereby “untethering” my spinal cord and restoring CSF (“Cerebral Spinal Fluid”) circulation.
Dr. Xu Xiao-Ming, Professor of Neurological Surgery at Indiana University, expresses the strategic surgical concept as follows: “The key goal here is restoration of spinal morphology.”
Put another way, the goal was to restore my spinal cord as close as possible to its original design and orientation within the spinal canal. That means my spinal cord would no longer be compressed by the large cyst nor would it tethered by strands of scar tissue left behind from my original spinal fusion surgery.
Instead, my spinal cord would be floating free again with full CSF circulation — free once again, as Dr. Zhu Hui expresses it more poetically, to “dance” with the rhythms of my heartbeat and breathing.
🙂
After the cyst had been cut and tethering scar tissue removed, the Dura mater was sutured back together. Key here is that the Dura Mater not leak CSF after it is sewed back together!
Finally, there’s an obvious need to build a frame around the access “door” had been cut open to access my spinal cord. This required the installation of titanium rods and screws – two vertical rods and one horizontal rod to provide lateral rigidity, held in place by six screws.
Then my neck muscles were pulled back over the titanium framework, and finally the surgeons sutured my skin back in place.
Summing up:
The surgery could not have gone more smoothly and, in my opinion, it was a remarkable success.
Indeed, given how fast my breathing was failing just one year ago, I can highly recommend patients who are have cysts, tethering issues, or any other spinal cord complication to come to Kunming to work with Dr. Zhu and Dr. Liu for surgery. I really had a world-class surgical team, and I don’t think you will find better or more experienced neurosurgeons anywhere in the world.
While I am an enthusiastic advocate for spinal surgery here in Kunming, full disclosure requires that I devote the next two blog posts to also discussing my immediate postsurgical care and some of the nightmares we had to endure in addition to long-term postsurgical challenges I have undergone over the past year. So this is a complicated story that I’ll lay out as clearly as possible.
Surgery Pictures
For readers who missed my earlier blog entry with the surgery pictures, I have included illustrations below courtesy of one of my physical therapists who routinely photographs and videos major surgical procedures in Kunming

The surgical team getting ready for surgery

This diagram illustrates the numerous layers surrounding the spinal cord. Dr. Liu had to drill away the bone of three vertebral lamina (C-5 through C-7) to gain wide “barn door” access to my spinal cord. Then in order to secure my spinal column at the end of the surgery, Dr. Liu used part of the vertebrae he had cut away, crushed up to make a sort of mortar, to reinforce positioning of the three titanium rods and six screws he used to stabilize my spinal column.

Before the dura mater is opened … this is the scene

First a small puncture of the dura mater … and gusher!

The dura mater is now wide open, exposing the pia mater in order to gain access to the arachnoid cyst on the anterior side of the pia mater, and also revealing 2 small syrinx cysts just inside of the pia mater that were successfully drained.

My surgical team deep in concentration
Finally, there are two videos taken during my surgery. I have decided to post these on YouTube because they serve to illustrate a very important outcome of the surgery that could not be seen in a still photograph.
In the first video, note carefully that my spinal cord is not moving at all, being literally stuck in place by scar tissue and wedged in tightly by the big (3.5 cm) cyst.
Also very much worth observing is the absence of blood. Dr. Liu is one of the very top neurosurgeons in the world, and his mantra is “no blood” when working on an open spinal cord. On top of the Pia mater, you can actually see the tiny, delicate blood vessels that supply the spinal cord, and none of these have been nicked. I lost virtually no blood during the entire surgery.
In the second video, after the team have surgically drained the big cyst and cleared out the scar tissue, you can actually see that my spinal cord has started beating again in rhythm with my heartbeat. I learned that your spinal cord is supposed to pulse naturally with your heartbeat and breathing, but mine had unfortunately been frozen in place for over two years. 😦
Video 1: No movement of the spinal cord: http://www.youtube.com/watch?v=w2soHLDNiWY&feature=youtu.be
Video 2: Spinal cord is again pulsing with the beat of my heart: http://youtu.be/KW2s-eOMcD0
FINAL NOTE: I received many e-mails from my readers asking me if I could post a few pictures of the knee brace that I have had to use for physical therapy since my leg was broken. My leg brace is made in Germany and was custom-made to fit my leg. In my opinion the Germans make the most reliable orthopedic devices.